
{kind=link}
Survey Reveals Rising Concern Over Facial Fat Loss Following Weight Loss
A new research survey discovered that 65% of women are concerned about experiencing facial fat loss in the…


Dr Linda Simpson explores how the subtle signs of perimenopause often present first in the aesthetic clinic, challenging practitioners to look beyond cosmetic concerns and recognise the underlying physiological changes at play.
Menopause and perimenopause are hot topics at the moment, but often the first whispers of its arrival are within the walls of your aesthetic treatment room. Coming from a medical background, we have been trained to identify patterns of presentation, connect symptoms, consider underlying pathology and identify primary and secondary causes. And yet, within aesthetics, there is a subtle but important shift.
The consultation is less about pathology and more focused on correction of volume loss, skin quality, treatment of rhytids, and improvement of skin texture. Importantly, the broader clinical context is sometimes left unexplored. The patient and your consultation skills have not changed simply because the setting has. Here is where your superpower lies. These skills don’t suddenly disappear when presented with cosmetics problems.
Within your aesthetic treatment room, we are often presented with women requesting facial rejuvenation.
How many times have you heard the words “I feel like I have aged overnight”, “I look tired”, “I don’t feel like myself anymore”?
These are not unfamiliar complaints. They are delivered casually, framed as aesthetic dissatisfaction rather than any clinical concern. These patients are not seeking a diagnosis from you, they are asking for aesthetic treatment. However, they often do not realise that they are describing underlying the unfolding physiological processes. This is where your pattern recognition should be peaked because if we pause and listen, these are not just cosmetic observations. They are clinical cues. And it is here where your clinical judgement becomes paramount.
Within aesthetics, there is a tendency to separate appearance from physiology and view facial ageing, skin quality, and perceived decline as amenable to correction with procedures however as clinicians, we must take a holistic approach.
What are women truly saying?
Before you is a woman with rapid perceived ageing, skin dryness, fatigue and loss of confidence. This constellation of features in any other clinical environment would prompt consideration of an underlying biological cause. In this case… perimenopause transition.
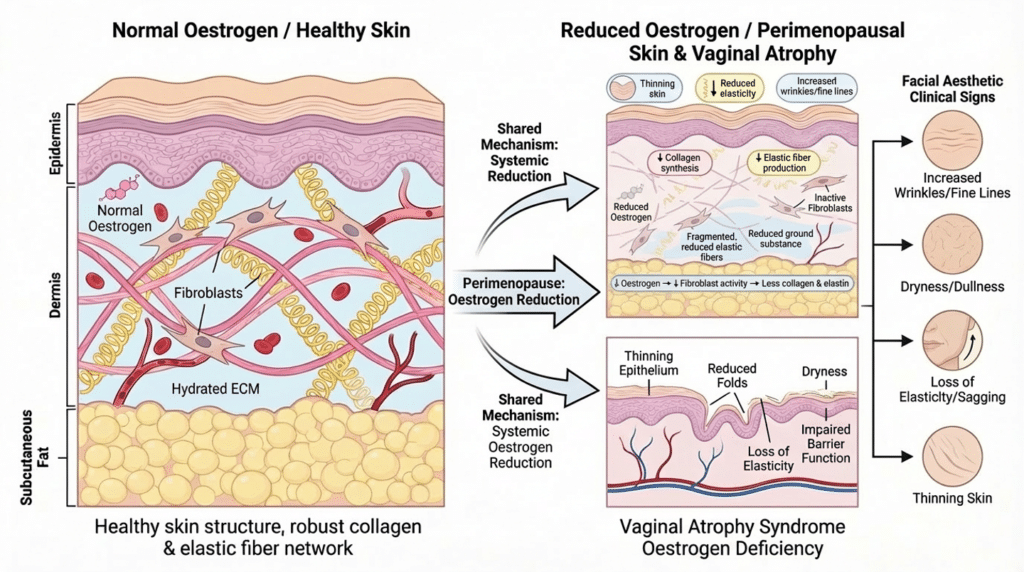
Perimenopause and menopause are not a cosmetic diagnosis. It is a biological transition where hormonal decline influences multiple organ systems such as the skin, urogenital tract and central nervous system. The face is therefore not ageing in isolation; it reflects what is taking place internally. Declining oestrogen contributes to reduced collagen production, decreased dermal thickness, impaired hydration, and loss of elasticity. All of which contribute to visible ageing. At the same time, women may experience vulvovaginal dryness, dyspareunia, urinary symptoms, sleep disturbance, anxiety, and cognitive changes.
These are not separate issues. They are different expressions of the same physiological shift. However, they are rarely presented together. Women often don’t state they are in perimenopause, instead they articulate what they see… changes in their face, hair, and skin. These are tangible, socially acceptable concerns. It is easier to say “I look tired” than disclose low libido, vaginal discomfort, or loss of identity. By contrast, low mood, cognitive change, sexual dysfunction, or genitourinary discomfort may be minimised, normalised or left unsaid.
As a result, the aesthetic consultation becomes the first place where these changes are voiced, even if indirectly. This places you, the practitioner in a unique position. We are not being asked to diagnose menopause within an aesthetic consultation, nor should we step beyond our scope of practice. We should however recognise patterns and open conversations. Ignoring signs does not maintain professional
boundaries, rather it bypasses clinical reasoning. What sets you apart is your ability to identify what you have been trained to recognise. The distinction here is between treating what is visible versus understanding what is driving it.
Aesthetic treatments have a valid and important role. Dermal fillers, skin boosters, and regenerative therapies can improve skin quality, restore volume, and enhance confidence. For many patients, this is meaningful and appropriate. However, these interventions do not address the underlying hormonal changes.
When treatments are delivered without context, there is a risk of creating a cycle in which patients pursue repeated procedures in an attempt to correct what in reality, is a systemic process.
Expectations may become unrealistic, and outcomes, although technically successful, may feel insufficient. This isn’t a failure of treatment and assessment; it’s a fundamental failure of framing. Clinical awareness ultimately allows us to shift that framing.
Recognising a potential menopausal pattern does not require formal diagnosis. It requires observation, listening, and the confidence to acknowledge what may be contributing to the presentation. In practice, this may be as simple as opening the door to a broader conversation: “Sometimes these changes can be linked to hormonal shifts, particularly around midlife. Have you noticed any other changes recently?”
This shouldn’t feel like a medical overreach, rather it the implementation of good clinical practice. Patient autonomy is respected whilst offering context. It allows women to engage with the idea (or not) without feeling medicalised or dismissed. This may be the first time this conversation has been had and the connection made. The fundamental consideration of informed consent must be addressed. If we aren’t
currently addressing the underlying mechanism of ageing, is the patient truly consented?
In aesthetic medicine, consent is often focused on procedural risks and expected outcomes. However, if the underlying driver of change is not acknowledged, the patient’s understanding of her condition may be incomplete. She may believe that her concerns are entirely aesthetic and therefore expect aesthetic treatments to provide full resolution. This opens the door to unmet expectations and high dissatisfaction. This is not because your treatment was inappropriate rather that the problem was not fully understood.
Providing context won’t diminish the value of the aesthetic treatment. It will ultimately enhance it.
When patients understand that their experience may be part of a broader physiological transition, they are better able to make informed decisions. They may still choose treatment, but with expectations that are more realistic and grounded. Here, trust is built and loyal relationships forged. It also creates an opportunity for appropriate signposting.
Encouraging patients to speak with their GP, explore menopause support, or consider hormonal management when relevant does not detract from the aesthetic consultation. It reflects a more integrated approach to your care; one that recognises that aesthetic medicine does not exist in isolation from the rest of the body.
Ultimately, this comes back to professional identity. As medically trained practitioners, we do not stop being clinicians when we enter an aesthetic setting. Our diagnostic skills, our ability to recognise patterns, and our responsibility to consider underlying causes remain unchanged.
Menopause is not a cosmetic diagnosis. It should not be reduced to one. However, its early manifestations are frequently encountered in aesthetic practice, often before they are recognised elsewhere. This highlights the responsibility we have within the aesthetic room. The question, then, is not whether we should treat what we see. It is whether we are willing to see beyond it.
When a woman tells us she feels she has aged overnight, we can respond with a syringe, or we can pause, apply the same clinical reasoning we would in any other setting, and consider what her presentation is telling us. In many cases, it is telling us far more than we think.
Gain full access to peer-reviewed protocols, our extensive digital archive, and the Tri-annual print edition delivered to your clinic.
£
250
Per Year
Subscribe
Auto-renews annually. Cancel anytime.
Subscribe to our newsletter for the latest insights from the aesthetics industry.
Subscribe NowA new research survey discovered that 65% of women are concerned about experiencing facial fat loss in the…

Dermatology Aesthetic Nurses Association Ireland (DANAI) has announced the opening of early bird registration for its inaugural Aesthetics…

Leading distributor, Healthxchange has unveiled its new ‘Trust in Aesthetics’ campaign, a values-led initiative designed to champion the…

Performance beauty company, Evolus, has announced the European commercial launch of Estyme® — a new collection of injectable…

As peptide therapies grow in popularity, Dr Ben Coyle, GP & Aesthetics Doctor, at The Goldhill Clinic, explores…
The UK’s Medicines and Healthcare products Regulatory Agency (MHRA) has introduced improved safety warnings for all botulinum toxin…

Compounding pharmacy Roseway Labs has launched Statera, a new 12-week education-led weight management programme. As demand for treatments…

Harpar Grace International (HGI) has announced its expansion into the dental sector, unveiling a new commercial programme designed…

A new purpose-built surgical centre dedicated to skin cancer treatment and advanced dermatologic surgery is set to open…

AMANDA PEARSON With an extensive background in the corporate beauty industry and a passion for supporting business growth,…