

Global Study Reveals What Really Drives Aesthetic Patients
A study published in the Aesthetic Surgery Journal found that confidence, self-expression and self-care – not simply the…

Against this backdrop, ACE Group World is proud to introduce the Need to Know Series, a new collection of concise, authoritative publications designed to address the questions clinicians most frequently raise in practice.
These are the topics that sit at the intersection of clinical judgement, governance, ethics and law, the areas
where uncertainty can compromise confidence, consistency and ultimately patient safety.
Abstract
Prescribing is both a privilege and a responsibility. As non‑medical prescribing expands across clinical settings, healthcare professionals must understand the regulatory, legal, and professional distinctions between licensed, off‑label, and unlicensed medicines. This guide integrates both UK and Republic of Ireland (ROI) governance frameworks to support safe, effective, and defensible prescribing across jurisdictions.
Introduction
Aesthetic practice sits at the intersection of medicine, artistry, and patient-centred care. Unlike many areas of healthcare, aesthetic treatments frequently rely on the use of medicines outside the strict boundaries of their Summary of Product Characteristics (SPC). Botulinum toxin is a familiar example: widely used for cosmetic indications that fall outside its licensed Summary of Product Characteristics (SPC).
Both the UK and Ireland permit off‑label and unlicensed use when clinically justified, but the legal basis, regulators, and professional standards differ.
This reality means that aesthetic practitioners routinely operate within a framework where off-label and unlicensed medicine use is normal, accepted, and often essential to meet patient expectations and achieve safe, effective outcomes. However, this also places a heightened professional responsibility on prescribers and those administering treatments. Understanding the legal, regulatory, and ethical distinctions between licensed, off-label, and unlicensed medicines is therefore not optional, it is a core component of safe aesthetic practice.
1. What Do We Mean by “Licensed” and “Unlicensed”?
Licensed medicine:
A licensed medicine has a UK marketing authorisation granted by the MHRA under the Human Medicines Regulations 2012 (HMR 2012). This authorisation confirms that medicine has met the required standards of quality, safety, and efficacy for specific, approved uses. (MHRA 2023).

Legal basis:

The license (marketing authorisation) specifies
Prescribing within these parameters is considered on-label use.
A licensed medicine has a marketing authorisation granted by the HPRA or the EMA under:
Ireland follows EU medicines law, unlike the post‑Brexit UK.
The license (marketing authorisation) specifies
Prescribing within these parameters is considered on-label use.
A licensed medicine has a marketing authorisation granted by the HPRA or the EMA under:
Ireland follows EU medicines law, unlike the post‑Brexit UK.
Off-label medicine:

A licensed medicine that is used outside the terms of its Summary of Product Characteristics (SPC). This may include using medicine for a different indication, dose, frequency, route, patient group, or anatomical area than those specified in its license.
Botulinum toxin is one of the most widely used medicines in aesthetic practice, yet only a small number of cosmetic indications are included within its marketing authorisation. For example, improvement of glabellar frown lines in adults could be the licensed use, however, in routine aesthetic practice, practitioners commonly administer botulinum toxin to other facial areas such as:
These uses fall outside the Summary of Product Characteristics (SPC) because they are not part of the medicine’s approved indications. This makes them off-label, even though they are widely accepted, evidence-supported, and considered standard practice within the aesthetics sector.
Off-label use is entirely legitimate when:
Ireland does not legislate off‑label use directly. Instead, it is governed by professional standards:
Off‑label use is permitted when:
Unlicensed medicine:
Medicine is unlicensed when it has no UK or Irish marketing authorisation.
Legal and regulatory basis:

Examples include:
Ireland: “Exempt Medicinal Products (EMPs)”
Governed by:
Pharmacies must notify the HPRA when supplying an EMP.
2. Professional and Legal Responsibilities Regulatory Framework
Prescribers must comply with:

Legislation
Regulatory and Professional Standards
Accountability
When prescribing unlicensed medicine, the prescriber assumes greater personal accountability for:
Regulatory support:
You must be able to demonstrate that your decision is:
Prescribers must comply with:
Doctors may prescribe unlicensed medicines freely; nurse and pharmacist prescribers must operate within Collaborative Practice Agreements (CPAs).
3. When Is It Appropriate to Prescribe Unlicensed Medicines?
Unlicensed prescribing may be appropriate when:
Regulatory support:
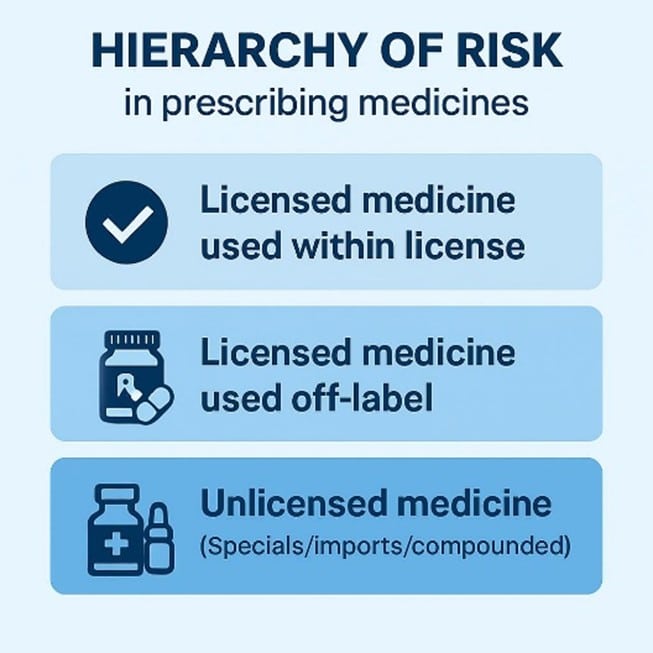
Prescribers must always consider the hierarchy of risk – Supported by MHRA (2025), GMC (2021), and RPS (2021).
Unlicensed medicines (EMPs) may be used when:
Governed by Article 5(1) EU Directive 2001/83/EC.
4. Informed Consent and Shared Decision-Making
When prescribing an unlicensed medicine, you must:
Regulatory support:
Patients do not need to sign a separate consent form, but clear documentation is essential.
5. Documentation and Governance
Good documentation protects both the patient and the prescriber. Record:
Regulatory support:

Ireland does not use the Yellow Card system.
Follow local policies on formularies, specials procurement, medicines governance, and incident reporting.
Who Can Prescribe Unlicensed Medicines?

In the UK, any appropriately qualified and authorised prescriber may prescribe unlicensed medicine, provided they take full clinical and professional responsibility for the decision. This includes both medical and non-medical prescribers.
Doctors: May prescribe unlicensed medicines when clinically appropriate (GMC, 2021).Dentists: May prescribe any medicine listed in the British National Formulary (BNF) on a private prescription. However, they must only prescribe medicines for identified dental needs, not general medical conditions.
Nurse Independent Prescribers (NIPs): May prescribe unlicensed medicines within competence and governance frameworks (NMC, 2023; MHRA, 2022).
Pharmacist Independent Prescribers (PIPs): May prescribe unlicensed medicines within scope (RPS, 2021; MHRA, 2025).
Other Independent Prescribers: Physiotherapists, podiatrists, optometrists, therapeutic radiographers, and paramedics may prescribe unlicensed medicines unless restricted by profession-specific legislation.
Supplementary Prescribers
May prescribe unlicensed medicines if included in the Clinical Management Plan (CMP) (Department of Health, 2003).
In Ireland, prescribing authority is held by doctors, dentists, registered nurse prescribers, registered midwife prescribers, and more recently pharmacists for a limited set of common conditions.
Doctors: hold full prescribing authority,
Dentists: may prescribe medicines relevant to dental practice.
Nurse and midwife prescribers: registered with the NMBI and employed by a health service provider., can prescribe within the boundaries of a Clinical Practice Agreement and their defined scope.
Pharmacist prescribers: have more limited and highly restricted prescribing powers
Other professional groups: Ireland does not grant prescribing rights to the wider range of allied health professionals seen in the UK (e.g., paramedics, physiotherapists, podiatrists).
Across both jurisdictions, community prescribers are not permitted to prescribe unlicensed medicines.
7. Who Cannot Prescribe Unlicensed Medicines?

In the UK:
In Ireland
8. Practical Considerations for Prescribers
Before Prescribing
Check BNF, IMF, SPC, NICE, NCEC, CKS, and local formulary; review evidence; consider licensed options first; assess patient factors (BNF, 2024; NICE, 2024).
| Function | BNF (UK) | IMF (Ireland) | NICE (England & Wales) | NCEC (Ireland) |
| What it is | National medicines formulary | National medicines formulary | National evidence‑based guidance body | National clinical guideline programme |
| Primary purpose | Practical prescribing guidance | Practical prescribing guidance | Clinical guidelines, HTAs, quality standards | National clinical guidelines for Irish health system |
| Scope | Medicines, dosing, interactions, cautions, prescribing advice | Medicines licensed in Ireland, dosing, interactions, reimbursement | Clinical pathways, diagnostics, public health, cost‑effectiveness | Priority national guidelines (e.g., sepsis, early warning scores, maternity) |
| Regulatory alignment | MHRA | HPRA | NHS England, MHRA, UK frameworks | Department of Health (Ireland), HSE |
| Legal status | Authoritative but not statutory | Authoritative but not statutory | Some guidance mandatory, for NHS commissioning | National Clinical Guidelines are mandated for implementation |
| Geographic relevance | UK | Ireland | England & Wales (NI adopts selectively) | Ireland |
When Prescribing
Use the lowest-risk option, ensure informed consent, provide clear instructions, communicate with MDT.
After Prescribing
Monitor treatment effectiveness, review the patient regularly, and document all findings clearly. Report any suspected adverse reactions through the appropriate national system: in the UK via the MHRA Yellow Card Scheme (MHRA, 2024), and in Ireland via the HPRA adverse reaction reporting system, as Ireland does not use the Yellow Card scheme.
Regulatory support:
References

CPD 2 Points
Gain full access to peer-reviewed protocols, our extensive digital archive, and the Tri-annual print edition delivered to your clinic.
£
250
Per Year
Subscribe
Auto-renews annually. Cancel anytime.
Subscribe to our newsletter for the latest insights from the aesthetics industry.
Subscribe NowA study published in the Aesthetic Surgery Journal found that confidence, self-expression and self-care – not simply the…

BTL Ireland has officially opened its new headquarters in Dublin, marking a significant investment in the company’s continued…
A new clinical governance initiative has been developed by ACE Group World to help enhance emergency preparedness in…

The British Association of Medical Aesthetic Nurses (BAMAN) has welcomed the UK Government’s Call for Evidence on proposals…

Skincare brand CellDerma has announced a new distribution partnership with Church Pharmacy, strengthening the brand’s presence across the…

Leading pharmaceutical company Allergan Aesthetics, an AbbVie company, has announced that they have received approval from the European…

Leading Aesthetics distributor, Healthxchange, has been appointed the new UK and Ireland distributor for the Jeisys POTENZA Advanced…

British Association of Medical Aesthetic Nurses (BAMAN) has announced the return of its flagship cadaveric anatomy programme this…

The Regenerative Aesthetics Multidisciplinary Conference & Exhibition (RAMCE) is set to return for a day full of dedicated regenerative…

Clinical-stage biotechnology company Absci has announced positive interim results from the Phase 1 HEADLINE™ clinical trial an investigational…