
{kind=link}

Global Study Reveals What Really Drives Aesthetic Patients
A study published in the Aesthetic Surgery Journal found that confidence, self-expression and self-care – not simply the…

Dr Jayne Vaughan explores the evolving understanding of bruxism and examines the comparative roles of occlusal splints and botulinum toxin in its management.
Bruxism is a common, complex parafunctional activity with significant dental, musculoskeletal, temporomandibular and aesthetic consequences. Traditionally, occlusal splints have been the mainstay of treatment within dentistry. However, growing evidence challenges their ability to meaningfully alter bruxist activity beyond protection against tooth wear [1]. In contrast, botulinum toxin has emerged as a targeted neuromuscular intervention that directly reduces the excessive muscle activity associated with bruxism, with an expanding evidence base supporting its clinical efficacy [2].
This article will review the contemporary understanding of bruxism, its epidemiology, causes and clinical manifestations. Particular focus is given to the comparative roles of occlusal splints and botulinum toxin, incorporating both the literature and my own extensive clinical experience as a dentist and aesthetic practitioner. Surgical options for severe temporomandibular joint disorders (TMD) associated with bruxism are also discussed, with emphasis on appropriate patient selection and multidisciplinary care.
Introduction
Bruxism represents a significant clinical challenge across dentistry, medicine and aesthetic practice. I have treated patients with bruxism for nearly 30 years, initially through conventional dental approaches such as occlusal splints, and more recently with the neuromodulator Botulinum Toxin. Over time, both the clinical approach and the scientific understanding of bruxism have evolved considerably.
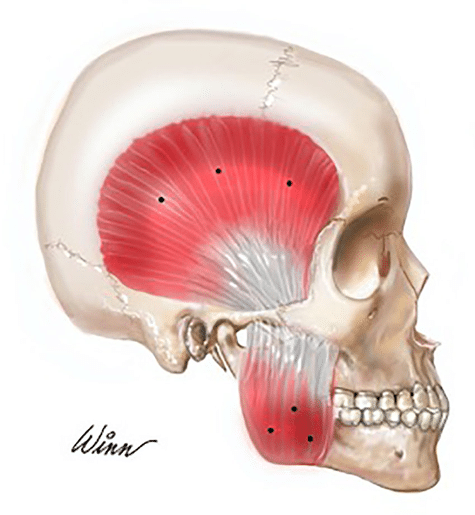
While occlusal splints remain widely prescribed, contemporary literature increasingly supports the view that they function primarily as to protect dental tissue rather than as definitive treatments for bruxism itself [3]. The broader aesthetic implication of chronic bruxism is masseter hypertrophy leading to an increased bigonial width, which is generally considered undesirable in females.
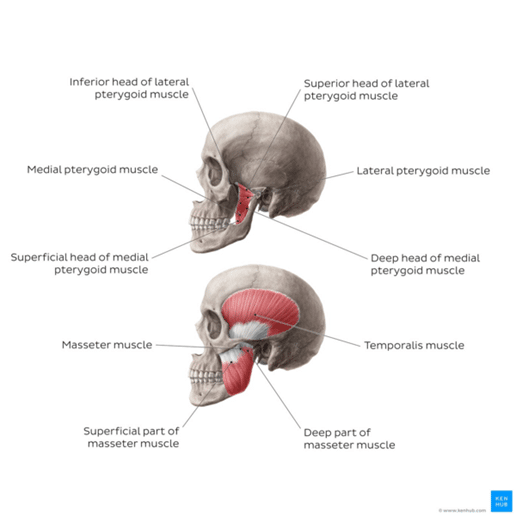
Fig. 1. Overview of the muscles of mastication, (Physiopedia, n.d.) [4]
Definition and Prevalence of Bruxism
Bruxism is common across all age groups, although prevalence varies according to age, sex and diagnostic criteria. Population studies estimate the overall prevalence of bruxism to range from approximately 8–31% in adults [5].
Bruxism is defined as a repetitive, involuntary activity of the muscles of mastication, characterised by clenching or grinding of the teeth and/or by bracing or thrusting of the mandible [1]. Current international consensus further makes the distinction between:
This distinction between sleep and awake bruxism is clinically important as they differ in their neurophysiological drivers, behavioural associations and treatment responses [1].
Aetiology and Contributing Factors
Bruxism is now widely regarded as a centrally mediated condition rather than one driven primarily by occlusal discrepancies [6]. This shift in understanding reflects growing evidence that peripheral occlusal factors are unlikely to be primary causes and may instead act as secondary or modifying influences. Contributing factors include dysregulation of central dopaminergic pathways involved in motor activity [7], psychological stress and anxiety, particularly in awake bruxism where clenching behaviours may occur during periods of heightened emotional tension [8], and sleep disturbances such as obstructive sleep apnoea, which can be associated with sleep-related bruxism episodes [9]. Certain medications, including selective serotonin reuptake inhibitors, have also been linked to the onset or exacerbation of bruxism [10]. In addition, evidence suggests a possible genetic susceptibility in some individuals [11].
These insights have practical implications for management. They support a move away from irreversible occlusal interventions as primary treatment strategies and favour a more conservative, individualised approach that considers behavioural, pharmacological, and sleep-related contributors alongside the management of dental and musculoskeletal consequences.
Clinical Presentation
Bruxism presents along a spectrum of severity, ranging from mild, often subconscious clenching/grinding to more significant dental and muscular consequences. Common clinical features include tooth wear, enamel fractures and restoration failure, dentine hypersensitivity, masticatory muscle pain and fatigue, tension-type headaches with associated neck or trapezius pain, and temporomandibular joint pain, clicking or restricted mouth opening [12].
From an aesthetic perspective, chronic masseter hypertrophy can significantly alter facial proportions, leading to a square or heavy lower facial appearance that (female) patients may find undesirable.
Overview of Treatment Modalities
Management of bruxism is typically multimodal and should be tailored to symptom severity, underlying causes, and patient expectations. Treatment may aim to protect dentition, reduce pain, address contributing behavioural or systemic factors, and, in selected cases, improve facial aesthetics [13]. No single modality is universally effective, and combination therapy is often required.
Behavioural and Conservative Approaches
Behavioural and conservative approaches frequently include patient education, stress reduction strategies, cognitive behavioural therapy, physiotherapy, jaw exercises, and optimisation of sleep hygiene [14]. These interventions are particularly relevant in awake bruxism, where parafunctional activity is often associated with psychological stress and heightened muscle tension [15]. While such approaches may reduce symptom severity, they are often insufficient in moderate to severe cases, especially where significant muscle hypertrophy, persistent pain, or dental damage is present [16].
Pharmacological (Non-injectable) Therapies
Pharmacological therapies utilise systemic agents including muscle relaxants and benzodiazepines in select cases [3]. However, evidence of sustained benefit is inconsistent, and their use is limited by sedation, dependency risk, and other adverse effects [17]. As a result, these medications are not recommended for long-term management and are typically reserved for short-term or acute symptom control.
Occlusal Splints – Night Guards
Occlusal splints remain widely prescribed in both bruxism and temporomandibular disorder (TMD). Proposed mechanisms include redistribution of occlusal forces, modification of proprioceptive input, protection of teeth and restorations from further mechanical wear. However, systematic reviews demonstrate no consistent evidence that splints reduce bruxist activity, pain intensity, or progression of TMD [6]. Their primary benefit appears protective rather than curative.
Importantly, splints do not address the central neuromuscular drivers of bruxism and may increase clenching activity in some patients. In my previous practice as a dentist, I regularly prescribed splints to protect dentition and restorations, however generally found their results variable. In addition, some patients found the splint itself difficult to tolerate, which in turn led to poor compliance.
In comparison to occlusal splints, my clinical experience indicates that Botulinum Toxin provides a more effective intervention for the management of bruxism. Administration of the toxin to affected muscles of mastication appears to target the neuromuscular drivers of the disorder, resulting in substantial symptomatic relief. In my practice, I have observed a near 100% rate of symptom alleviation and high levels of patient-reported satisfaction, highlighting its benefit as a reliable therapeutic option.
Botulinum Toxin in the Management of Bruxism
Botulinum toxin provides a targeted neuromuscular approach by reducing excessive muscle contraction while preserving function. Injected into the masseter and, where appropriate, temporalis muscles, it reduces bite force, muscle tenderness and bruxist activity [18].
Clinically, patients frequently report improvements in pain, headaches, sleep quality and facial comfort. A secondary, but often welcomed effect, is reduction in masseter hypertrophy and lower facial width. When administered correctly, botulinum toxin demonstrates a favourable safety profile [19].
How to Treat Bruxism with Botulinum Toxin: A Practical Guidance for Aesthetic Practitioners
Muscles Commonly Treated
The masseter is often the principal muscle implicated in bruxism-related clenching. Clinical assessment should include inspection for hypertrophy, palpation during clenching to confirm muscle bulk and activity, and evaluation of mandibular function. Injection into the lower third of the muscle is standard practice to minimise diffusion to adjacent structures. The temporalis may be treated when clinical findings indicate significant involvement, such as temporal pain, tenderness on palpation, or evidence of compensatory hyperactivity. Treatment should be guided by symptom distribution and functional examination rather than aesthetic considerations alone.
Injection of the medial pterygoid is reserved for refractory or complex cases where clinical assessment demonstrates persistent deep muscular involvement. Due to anatomical complexity and proximity to critical neurovascular structures, treatment of this muscle requires advanced anatomical knowledge and should be undertaken only by clinicians with specialist training in maxillofacial anatomy and procedural techniques.
Injection Technique and Sites
Ask the patient to clench to allow clear identification of the masseter. Mark out the anterior, posterior and inferior borders of the masseter. Draw a line from the tragus to the oral commissure. This represents the superior border of the target treatment area. As a guide, injections should be positioned at least 1cm within these boundaries to reduce the risk of toxin diffusion to the risorius muscle and damage to adjacent structures.
Ask the patient to clench again to palpate to locate the apex of maximal contraction. Using a 13 mm needle, administer injections at 3–5 points within the lower two-thirds of the masseter muscle belly, centred around this region of maximal bulk. Care should be taken to avoid the parotid gland posteriorly and the marginal mandibular branch of the facial nerve inferiorly.
Advance the needle until bony contact is achieved, then inject while withdrawing. This technique facilitates distribution across both the deep and superficial fibres of the masseter and reduces the risk of compensatory superficial bulging.
Temporalis injections should be placed within the anterior and middle thirds of the muscle, avoiding the superficial temporal vessels. As the temporalis inserts onto bone, injections are administered with the needle advanced to bony contact prior to injection.
Typical Dosing (per side, as a guide)
Doses should be individualised based on muscle bulk, symptom severity and prior response. Conservative dosing is advised initially, with review after 2 weeks to assess therapeutic effect and the need for adjustment.
Treatment may be repeated after 12 weeks, however many patients feel the effects of the treatment last longer than this, up to 6 months in some cases.
Fig 2. Injection sites for Bruxism. (Bouloux, 2022) [20]
Risks of Botulinum Toxin Treatment for Bruxism
Botulinum toxin type A injections for bruxism are generally considered safe in doses typically used for masseter and temporalis muscles, but adverse effects are described and should inform clinical consent and risk mitigation.
In recent systematic reviews, reported side effects were mostly mild and transient, including injection site discomfort, temporary changes in smile or facial expression, and chewing difficulty, with rates of up to ~15–20% in some trials; these effects typically resolved without long-term sequelae. More rarely, masticatory weakness, headache, asymmetrical muscle effects, or limited mouth opening have been observed, particularly when toxin diffuses into adjacent muscles or with higher doses.
Emerging observational data also suggests a possible association between repeated neuromodulator use and mandibular bone changes, although the clinical significance remains under investigation. These findings underscore the importance of precise injection technique, conservative dosing, and thorough patient counselling regarding common transient adverse events and less frequent but clinically relevant outcomes [21].
Recognising Bruxism and TMJ Conditions Amenable to Botulinum Toxin
Key features suggesting a favourable response include:
Atypical or Poor Responders to Botulinum Toxin
Not all facial pain or TMD is bruxism-driven. Poor responders may include:
Accurate diagnosis is essential to prevent inappropriate treatment and unmet expectations. In my clinical experience, some atypical patients may still elect to proceed with botulinum toxin therapy following comprehensive examination. However, they should be clearly advised of, and consent to, the greatly reduced likelihood of success.
Surgical Options in Severe TMD Associated with Bruxism
In a minority of patients, chronic bruxism contributes to severe, refractory TMD requiring surgical intervention.
Minimally Invasive Procedures (Ângelo et al., 2024)
Open Joint Surgery
Open procedures, including disc repositioning, discectomy or joint reconstruction, are reserved for severe structural disease [28].
These interventions address joint pathology rather than bruxism itself and should be undertaken within a multidisciplinary framework [29].
Clinical Takeaways
Conclusion
Bruxism is a prevalent and complex condition with significant functional and aesthetic implications. Contemporary evidence supports a shift towards neuromuscular interventions, particularly botulinum toxin, for appropriately selected patients. Surgical options remain reserved for severe, refractory TMD. A thoughtful, evidence-informed and individualised approach is essential.
References
Email editor@theaestheticsmagazine.com to receive your CPD certificate.

Gain full access to peer-reviewed protocols, our extensive digital archive, and the Tri-annual print edition delivered to your clinic.
£
250
Per Year
Subscribe
Auto-renews annually. Cancel anytime.
Subscribe to our newsletter for the latest insights from the aesthetics industry.
Subscribe NowA study published in the Aesthetic Surgery Journal found that confidence, self-expression and self-care – not simply the…

BTL Ireland has officially opened its new headquarters in Dublin, marking a significant investment in the company’s continued…
A new clinical governance initiative has been developed by ACE Group World to help enhance emergency preparedness in…

The British Association of Medical Aesthetic Nurses (BAMAN) has welcomed the UK Government’s Call for Evidence on proposals…

Skincare brand CellDerma has announced a new distribution partnership with Church Pharmacy, strengthening the brand’s presence across the…

Leading pharmaceutical company Allergan Aesthetics, an AbbVie company, has announced that they have received approval from the European…

Leading Aesthetics distributor, Healthxchange, has been appointed the new UK and Ireland distributor for the Jeisys POTENZA Advanced…

British Association of Medical Aesthetic Nurses (BAMAN) has announced the return of its flagship cadaveric anatomy programme this…

The Regenerative Aesthetics Multidisciplinary Conference & Exhibition (RAMCE) is set to return for a day full of dedicated regenerative…

Clinical-stage biotechnology company Absci has announced positive interim results from the Phase 1 HEADLINE™ clinical trial an investigational…