
{kind=link}

Global Study Reveals What Really Drives Aesthetic Patients
A study published in the Aesthetic Surgery Journal found that confidence, self-expression and self-care – not simply the…


Emma Heaney shares why conventional microneedling remains the safer, evidence-based first-line treatment for skin rejuvenation, while radiofrequency microneedling should be reserved for carefully selected cases due to its higher risk profile.
INTRODUCTION
Microneedling (MN) is a cornerstone treatment in aesthetic dermatology, inducing dermal regeneration through controlled micro-injury and fibroblast activation.¹ Its indications include acne scarring, fine lines, and dyschromia, with consistent outcomes and minimal downtime.²
Radiofrequency microneedling (RFMN) combines microneedle penetration with thermal energy delivery to enhance collagen contraction.³ However, thermal injury introduces increased procedural risk and variability in outcomes.
METHODS
A structured narrative review of PubMed-indexed literature was conducted, including systematic reviews, meta-analyses, and randomised controlled trials. Only peer-reviewed academic sources were included.
MECHANISMS OF ACTION
Conventional Microneedling MN induces a wound-healing cascade via growth factor release (TGF-β, PDGF, FGF), stimulating fibroblast activity and collagen synthesis.¹
Radiofrequency Microneedling
RFMN adds thermal coagulation, leading to collagen denaturation and contraction. However, thermal diffusion increases the risk of unintended tissue injury.³ ⁴
(Figure 1,2,3)
CLINICAL OUTCOMES
Conventional Microneedling
MN demonstrates consistent improvement in acne scarring and skin quality. Meta-analysis data shows ~83% patient satisfaction with low complication rates.²
Conventional Microneedling (MN):
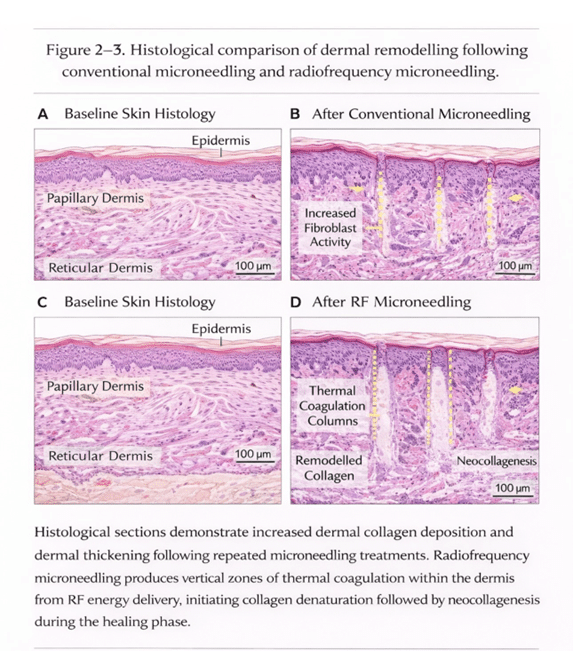
•Acne Scarring: MN consistently improves rolling and boxcar scars. Meta-analysis data (21 studies, n=723) shows ~83% patient satisfaction.² Histology demonstrates increased dermal thickness and type I/III collagen deposition.² ⁸
•Fine Lines & Wrinkles: Multiple RCTs show significant reduction in superficial rhytides, especially when combined with adjunctive therapies like PRP or polynucleotides.² ⁶ ¹⁰
•Pigmentary Disorders: MN has a mild effect on dyschromia, with improved uniformity of skin tone observed in several prospective studies.² ⁹
•Skin Texture & Pore Size: Studies report improvements in epidermal smoothness and decreased pore size, likely due to neocollagenesis and elastin remodeling.² ⁸
•Patient Satisfaction & Downtime: High satisfaction rates correlate with low complication rates. Transient erythema typically resolves within 24–48 hours.²
Radiofrequency Microneedling
RFMN is effective for certain indications but does not consistently outperform MN, particularly in superficial dermal conditions.³
•Acne Scarring: RFMN may improve deeper scars more effectively than MN in some cases, but results are variable and highly dependent on device settings and operator technique.³ ⁴
•Skin Laxity: Some studies show improved dermal tightening due to collagen contraction from thermal energy, particularly in mid-to-deep dermis.³ ⁴
•Pigmentary Disorders & Fine Lines: Evidence does not consistently show superiority over MN for superficial wrinkles or pigmentation.³ ⁴
•Treatment Variability: Outcomes are more heterogeneous than MN alone, with patient-specific responses influenced by skin type, scar depth, and energy parameters.³ ⁴
•Patient Experience: Higher procedural discomfort is reported, often requiring topical anaesthesia or cooling, and satisfaction rates are slightly lower due to increased risk of adverse events.³ ⁴
SAFETY PROFILE
Conventional Microneedling (MN): Well tolerated, with transient erythema and minimal downtime.¹ ²
•Common Adverse Events: Mild erythema, edema, and pinpoint bleeding are expected and transient.¹ ²
•Infection Risk: Rare when aseptic technique is followed; no systemic complications reported in large series.² ⁹
•Pigmentary Changes: Minimal risk; post-inflammatory hyperpigmentation is uncommon and mostly reported in Fitzpatrick IV–VI skin types.²
•Downtime & Recovery: Minimal, allowing rapid return to normal activities; often 24–48 hours.¹
•Long-Term Safety: No evidence of fat atrophy, scarring, or permanent nerve injury with standard MN protocols.¹ ²
Radiofrequency Microneedling (RFMN):
Associated with increased risk including burns, hyperpigmentation, scarring, fat atrophy, and nerve injury.³ ⁴
•Thermal Risks: Burns, blistering, or scarring can occur if settings are too high or applied unevenly.³ ⁴
•Pigmentary Complications: Post-inflammatory hyperpigmentation or hypopigmentation reported, particularly in darker skin types (Fitzpatrick IV–VI).³ ⁴
•Structural Complications: Rare reports of fat atrophy and localized nerve injury exist, especially when high energy or deep penetration is used.³ ⁴ ¹⁴
•Downtime & Discomfort: Often greater than MN alone, with erythema and edema lasting 2–5 days; topical anaesthesia usually required.³ ⁴
•Operator Dependence: Safety and efficacy are highly dependent on practitioner experience, device calibration, and patient selection.³ ⁴
(Table 1 )
FDA SAFETY CONSIDERATIONS (2025)
Regulatory Considerations: The FDA (2025) has issued safety communications emphasizing that RFMN devices can cause serious adverse events, including burns, scarring, fat loss, and nerve injury.⁵ Clinicians should weigh benefits against risk, particularly in superficial skin indications where MN alone is sufficient.
ADJUNCTIVE AND COMBINATION THERAPIES
“STACKED PROTOCOLS”
Stacked protocols centred on microneedling areincreasingly supported by evidence.⁶ ⁷ ¹³ MN enhances transdermal delivery, allowing integration of regenerative therapies:
• PRP → improved scar outcomes (RCT evidence)⁶ ⁷
• Polynucleotides → fibroblast stimulation¹⁰
• Exosomes → emerging regenerative signalling¹¹
• LED → reduced inflammation⁹
RFMN induced thermal effect alters tissue response and can modulate transdermal absorption, sometimes limiting passive adjunct delivery compared with conventional microneedling, and may carry a higher risk of heat related side effects when combined with certain stacks. ¹⁴
CONCLUSION
Microneedling remains the first-line treatment for skin rejuvenation due to consistent efficacy and safety.¹ ² RFMN is effective but introduces greater risk and variability, without consistent superiority.³ ⁴
FUTURE DIRECTIONS
Further high-quality comparative studies and long-term safety data are required to optimise treatment selection and standardise clinical protocols.
Figure 1 Mechanism of Action
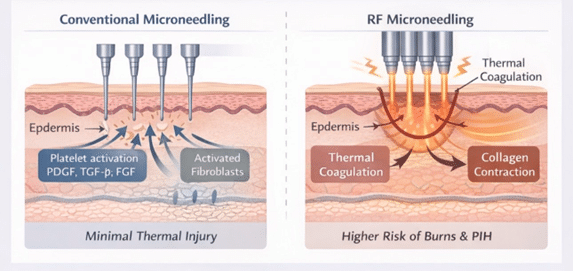
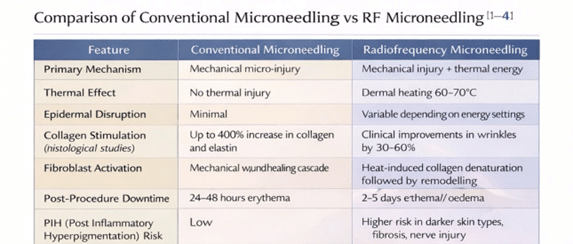
Table 1
References
1. Jaiswal S, et al. Microneedling in dermatology: A comprehensive review of applications, techniques, and outcomes. Cureus. 2024.
2. Aust MC, et al. Percutaneous collagen induction therapy: An alternative treatment for scars, wrinkles and skin laxity. Clin Cosmet Investig Dermatol. 2008.
3. Wang Q, et al. Radiofrequency microneedling applications in dermatology: A scoping review. Aesthetic Plast Surg. 2025.
4. Kong SH, et al. Clinical outcomes of radiofrequency microneedling for acne scars and skin laxity. Dermatol Surg. 2024.
5. U.S. Food and Drug Administration. Safety Communication RF microneedling devices and reported adverse events. 2025.
6. Alam M, et al. Microneedling combined with PRP for acne scars: A randomized controlled trial. JAMA Dermatol. 2014.
7. Fabbrocini G, et al. Microneedling in scar treatment: Clinical outcomes and histology. Dermatol Ther. 2009.
8. Majid I. Percutaneous collagen induction therapy in skin rejuvenation: Randomized study. J Cutan AesthetSurg. 2009.
9. Dogra S, et al. Safety and efficacy of microneedling: Prospective study. Dermatol Surg. 2014.
10. Lee HJ, et al. Polynucleotide-based regenerative treatments in dermatology. Aesthetic Surg J. 2025.
11. Zhang Y, et al. Exosome therapy in dermatology and regenerative medicine. Regen Med. 2024.
12. Avci P, et al. Low-level laser and LED photobiomodulation in dermatology. Semin Cutaneous Med Surg. 2013.
13. Fabbrocini G, et al. Microneedling and combination therapies: Evidence review. Clin Cosmet Investig Dermatol. 2018.
14. Goldberg DJ. Adverse effects and risk management in RF microneedling. Dermatol Surg. 2022
Gain full access to peer-reviewed protocols, our extensive digital archive, and the Tri-annual print edition delivered to your clinic.
£
250
Per Year
Subscribe
Auto-renews annually. Cancel anytime.
Subscribe to our newsletter for the latest insights from the aesthetics industry.
Subscribe NowA study published in the Aesthetic Surgery Journal found that confidence, self-expression and self-care – not simply the…

BTL Ireland has officially opened its new headquarters in Dublin, marking a significant investment in the company’s continued…
A new clinical governance initiative has been developed by ACE Group World to help enhance emergency preparedness in…

The British Association of Medical Aesthetic Nurses (BAMAN) has welcomed the UK Government’s Call for Evidence on proposals…

Skincare brand CellDerma has announced a new distribution partnership with Church Pharmacy, strengthening the brand’s presence across the…

Leading pharmaceutical company Allergan Aesthetics, an AbbVie company, has announced that they have received approval from the European…

Leading Aesthetics distributor, Healthxchange, has been appointed the new UK and Ireland distributor for the Jeisys POTENZA Advanced…

British Association of Medical Aesthetic Nurses (BAMAN) has announced the return of its flagship cadaveric anatomy programme this…

The Regenerative Aesthetics Multidisciplinary Conference & Exhibition (RAMCE) is set to return for a day full of dedicated regenerative…

Clinical-stage biotechnology company Absci has announced positive interim results from the Phase 1 HEADLINE™ clinical trial an investigational…