

Global Study Reveals What Really Drives Aesthetic Patients
A study published in the Aesthetic Surgery Journal found that confidence, self-expression and self-care – not simply the…


Nurse practitioner Patricia Molloy draws on 12 years of clinical experience to explore the science, indications and patient selection considerations behind two of aesthetics’ most widely used dermal filler categories.
The landscape of aesthetic medicine is evolving rapidly. As patient demand shifts toward treatments that deliver not only immediate cosmetic improvement but also longer-term skin health benefits, practitioners are increasingly required to navigate a growing and sophisticated portfolio of dermal filler options.
Central to this decision-making process is understanding the fundamental differences between two distinct categories of injectable treatment: hyaluronic acid (HA) fillers and collagen-stimulating fillers, specifically those based on polycaprolactone (PCL).
In this article, nurse practitioner Patricia Molloy, who brings 12 years of clinical experience with PCL-based fillers, explores the science underpinning both treatment categories, examines their respective indications and contraindications, and shares her clinical approach to patient and product selection.
Illustrated with real-world case studies, this article aims to provide practitioners with a practical, evidence-based framework for integrating both HA and PCL fillers into their treatment repertoire – ensuring outcomes that are not only aesthetically compelling, but tailored precisely to each individual patient’s needs.
Collagen Stimulator Fillers
Collagen stimulator fillers are made of microspheres of either Polycaprolactone (PCL), Calcium Hydroxyapatite (CaHA), or Poly-L-Lactic acid (PLLA), all suspended in a carrier gel. They all act in a similar way, initially acting as a volumising filler and then acting as a collagen stimulator.
In comparison, I have selected the polycaprolactone (PCL)-based product, with which I now have 12 years of clinical experience in patient treatment. This filler is composed of a unique patented formulation comprising 70% carboxymethyl cellulose (CMC)-based gel carrier and 30% PCL microspheres.
The PCL microspheres are maintained in a homogeneous suspension within the CMC-based gel carrier. Both PCL and CMC demonstrate excellent and well-established biocompatibility profiles.¹
Properties of CMC
CMC is a natural material derived from cellulose; it is not cross-linked and is nontoxic. It is a recognised pharmaceutical excipient. Its other properties include:
Properties of PCL
PCL is a non-toxic medical polyester, first synthesised in the early 1930s. It is attractive for use in dermal fillers because of its ease of bioresorption, and it is naturally hydrolysed into carbon dioxide and water within the body.²
The PCL microspheres are designed to offer optimal biocompatibility. They have a smooth surface, a spherical shape and a size of approximately 25–50 μm.¹
PCL has an excellent safety profile and has been used in the biomedical field for more than 70 years in a range of applications, from sutures to tissue, and recently for organ replacements by 3D printing. It is also used in CE-marked and US FDA-approved products.²
The physical properties of this filler differ from those of other dermal fillers on the market in three key ways:³,⁴,⁵
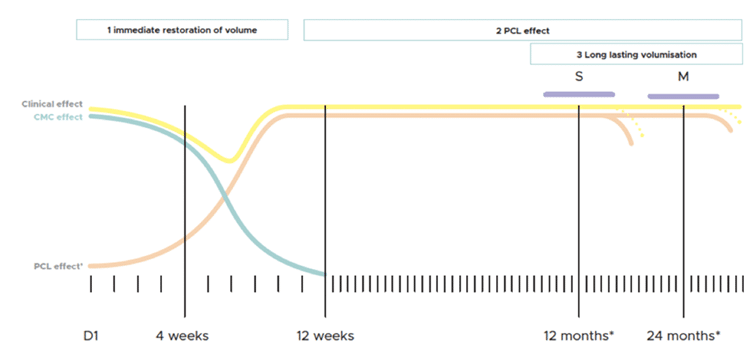
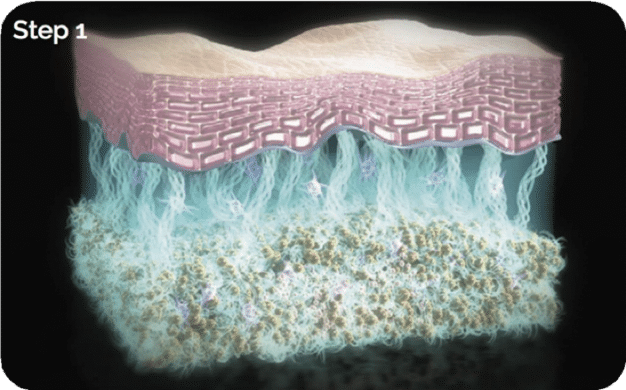
It has two distinct phases of activity:
Step 1: Immediately after injection, the CMC component provides temporary volume, which gradually decreases over 2–3 months.
Step 2: The PCL microspheres induce neocollagenesis of types I and III collagen, with more persistent type I collagen structure gradually increasing over 1–3 months and the PCL microspheres becoming embedded in the type I collagen scaffold.
The resulting collagen volume replaces the initial volume increase caused by the CMC gel. The collagen scaffold stimulated by the PCL microspheres persists after they have been resorbed, leading to a durable volume increase.

PCL gel’s elasticity is greater than that of volumising hyaluronic acid (HA), meaning that projection and volumisation of the injected area are instantly visible. Because the collagen-stimulating PCL microspheres are maintained in the injection area, aesthetic improvement is also more long-term than that seen with HAs.⁶
It also has excellent rheological properties and combines high elasticity with specifically designed viscosity that is suitable for subdermal injection.²
In a randomised, prospective, blinded, split-face, single-centre study comparing PCL with HA in 40 patients, nasolabial folds (NLFs) treated with PCL showed statistically significant improvements on the Wrinkle Severity Rating Scale, and greater improvements on the Global Aesthetic Improvement Scale when compared with NLFs treated with an HA-based dermal filler.⁶
PCL also improves skin quality, enhancing density, firmness, tonicity and texture from within. A clinical trial was carried out to assess the effect of PCL on skin quality parameters in 24 patients up to 24 months post-treatment. Although PCL was injected in the subdermis of the midface, patient echographs clearly showed a substantial increase in tissue density in the dermis following treatment with PCL, compared with baseline.⁷
This improvement was statistically significant at all time points during the 24-month study. Skin firmness, tonicity and smoothness were also statistically significantly improved with PCL compared with baseline.⁷
Hyaluronic Acid Fillers
HA-based dermal fillers are composed of a biocompatible, synthetic gel made from linear polysaccharide chains, often cross-linked with BDDE (1,4-butanediol diglycidyl ether) for longevity. These fillers typically include water for hydration, high-molecular-weight HA to attract water for volume, and often lidocaine to reduce pain during injection.
Clinical Experience with Collagen Stimulating Fillers and Hyaluronic Fillers
Patient and product selection is dependent on a full patient skin assessment, medical history and the patient’s needs.
Why Collagen Stimulating Fillers?
Why Hyaluronic Acid Filler?
As previously discussed, the rheology makes it easy to understand the beautiful, natural treatments that can be achieved with HA.⁸ The key characteristics include:
Indications for Hyaluronic Acid Fillers
Initially, I always carry out a comprehensive consultation to educate the patient on the products and how they perform in the skin. Depending on the patient’s medical history, preference, and my guidance, a filler is selected.
In some cases, a combination of both may be used. If improving skin quality is the goal, PCL is the preferred choice, but if treating the tear trough and lips in the same patient, HA would be used in those areas.
Both give a very natural and effective result. However, the decision to use either, or both, will depend on the patients’ expectations and the effect needed.
Why select PCL?
Why select HA?
Case Study 1: PCL
A 58-year-old female patient presented with deep nasolabial folds and pronounced marionette lines. PCL was used to address the lower face with a subdermal threading technique via a 25G cannula: nasolabial folds received 0.3 mL delivered as subdermal linear threads, and marionette lines and prejowl sulcus received 0.7 mL delivered as subdermal linear threads. Immediate structural support was achieved, with visible improvement in tissue support and a noticeable softening of the marionette region.⁶

Before After
Case Study 2: HA

Patient:
A 33-year-old female patient presented for non-surgical rhinoplasty.
Treatment:
Hyaluronic acid (HA) filler was administered in the midline using a 30G needle. Two 0.05 mL periosteal bolus injections were placed along the midline dorsum, followed by a single 0.1 mL injection to the nasal tip.
Outcome:
The treatment achieved a noticeable improvement in nasal contour, and the patient reported a high level of satisfaction with the result.
Case Study 3: HA

Patient:
A 38-year-old female patient presented seeking subtle, natural-looking facial rejuvenation.
Treatment:
A full-face hyaluronic acid (HA) treatment plan was performed to restore volume, improve structural support and achieve balanced rejuvenation.
Clinical considerations:
The tear troughs were not treated, as the patient demonstrated poor lacrimal drainage with associated fluid retention, making this area unsuitable for treatment and therefore contraindicated.
Conclusion
Both PCL and HA are unique, safe and effective dermal fillers.²,⁸ The decision of which to use should be determined by the patient’s skin condition, age, areas to be treated and patient’s expectations. HA will provide the patient with immediate results, whereas PCL will provide a long-term, regenerative collagen-stimulating treatment.²,⁶ These two products give the ability to achieve measurable results and increase patient satisfaction.⁷
References
¹ Nicolau PJ, Marijnissen-Hofsté J. Neocollagenesis after injection of a polycaprolactone based dermal filler in a rabbit. Eur J Aesth Med Dermatol. 2013;3:19–26.
² Christen M, Vercesi F. Polycaprolactone: How a well-known and futuristic polymer has become an innovative collagen-stimulator in aesthetics. Clin Cosmet Investig Dermatol. 2020;13:31–48.
³ Anderson JM. Mechanisms of inflammation and infection with implanted devices. Cardiovasc Pathol. 1993;2(3):33–41.
⁴ Laeschke K. Biocompatibility of microparticles into soft tissue fillers. Semin Cutan Med Surg. 2004;23(4):214–217.
⁵ Nicolau PJ. Long-lasting and permanent fillers: Biomaterial influence over host tissue response. Plast Reconstr Surg. 2007;119(7):2271–2286.
⁶ Galadari H, Van Abel D, Nuami KA, Faresi FA, Galadari I. A randomized, prospective, blinded, split-face, single-center study comparing polycaprolactone to hyaluronic acid for treatment of nasolabial folds. J Cosmet Dermatol. 2015;14(1):27–32.
⁷ Moers-Capri MM, Sherwood S. Polycaprolactone for the correction of nasolabial folds: A 24-month, prospective, randomized, controlled clinical trial. Dermatol Surg. 2013;39:457–463.
⁸ Sinclair. MaiLi physician leaflet. 2021. Available from: https://sinclairprodbackend.azurewebsites.net/media/aaofhxv4/physcians-leaflet.pdf
⁹ Sinclair. Ellansé 10-year anniversary brochure. 2022. Available from: https://sinclairprodstorage.blob.core.windows.net/media/z4bdzreh/ellansé-an-experts-guide-digital-singles-2-00-stc-28mar22singles-1-27-1.pdf
Gain full access to peer-reviewed protocols, our extensive digital archive, and the Tri-annual print edition delivered to your clinic.
£
250
Per Year
Subscribe
Auto-renews annually. Cancel anytime.
Subscribe to our newsletter for the latest insights from the aesthetics industry.
Subscribe NowA study published in the Aesthetic Surgery Journal found that confidence, self-expression and self-care – not simply the…

BTL Ireland has officially opened its new headquarters in Dublin, marking a significant investment in the company’s continued…
A new clinical governance initiative has been developed by ACE Group World to help enhance emergency preparedness in…

The British Association of Medical Aesthetic Nurses (BAMAN) has welcomed the UK Government’s Call for Evidence on proposals…

Skincare brand CellDerma has announced a new distribution partnership with Church Pharmacy, strengthening the brand’s presence across the…

Leading pharmaceutical company Allergan Aesthetics, an AbbVie company, has announced that they have received approval from the European…

Leading Aesthetics distributor, Healthxchange, has been appointed the new UK and Ireland distributor for the Jeisys POTENZA Advanced…

British Association of Medical Aesthetic Nurses (BAMAN) has announced the return of its flagship cadaveric anatomy programme this…

The Regenerative Aesthetics Multidisciplinary Conference & Exhibition (RAMCE) is set to return for a day full of dedicated regenerative…

Clinical-stage biotechnology company Absci has announced positive interim results from the Phase 1 HEADLINE™ clinical trial an investigational…